Making human neurons from skin cells
Neurons are produced in the central nervous system during the embryogenesis and perinatal period. Passed this initial neurogenesis, neurons lost to trauma, disease or aging, are not being replaced. To date there is no technology that could force the brain to regenerate new neurons in vivo. However, there are genetic engineering technologies that can transform cell types such as skin cells into neurons, in vitro.
Prior to starting these genetic engineering manipulations, a source of skin cells is therefore required. Our company has developed its own proprietary method to cryopreserve skin biopsies for long distance shipping. Skin punch biopsies are easy to obtain, and once frozen with our special formulation, they retain the capacity for producing dermal fibroblasts, a subtype of skin cells, which become our principal source of cells for neural engineering. One single biopsy can generate a few million neurons.
The fibroblasts are then transformed into neurons by a technique called ‘direct reprogramming’ in vitro. This is by contrast to other techniques that require to first de-differentiate skin cells into Pluripotent Stem Cells before re-differentiating these PSC into neurons. Techniques that use pluripotent stem cell intermediates are therefore not direct, and upon reimplantation they almost always produce teratomas. Since our goal is to reimplant these neurons without inducing teratomas and tumors, our method bypasses pluripotency. This ‘pluripotent free’ approach has been achieved by other laboratories as well, proving that acquiring pluripotency is not required to generate neurons. Our method is also particular because no “DNA vectors” are used during genetic engineering. This prevents any possible insertional mutagenesis in the genome of the skin cells. Instead, we exclusively use RNAs, either for microRNA mimicry, RNA interference, RNA activation or for transfecting full transcripts. The results are shown below.
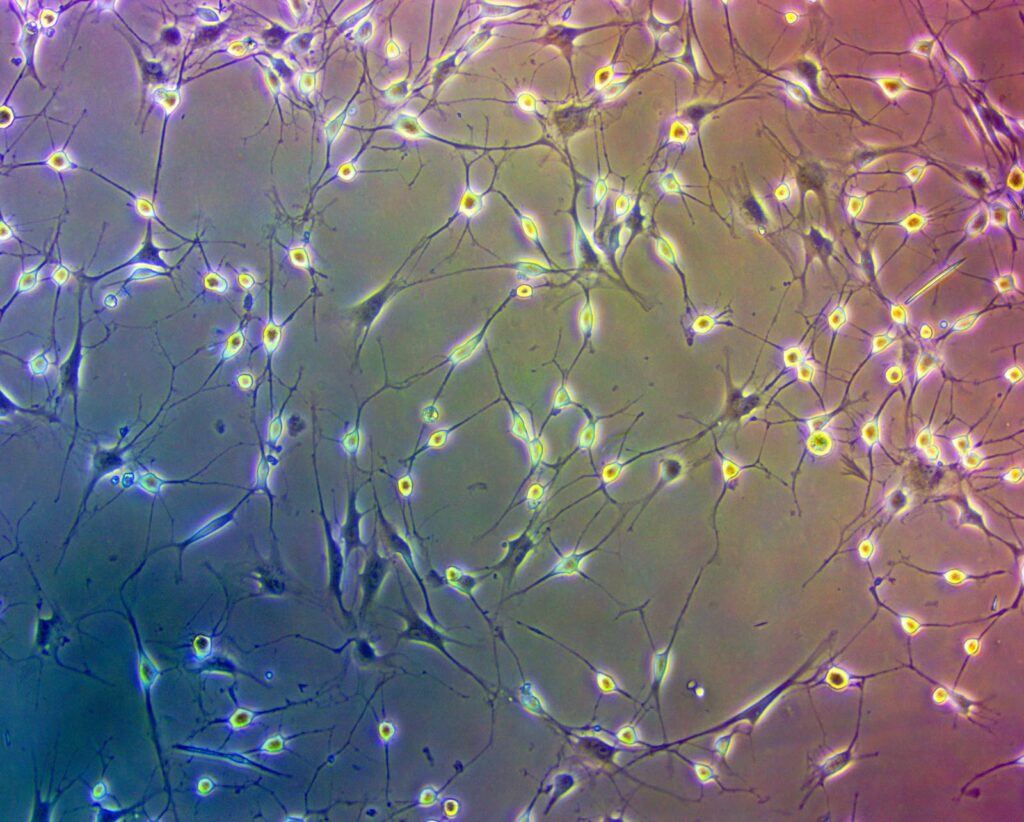
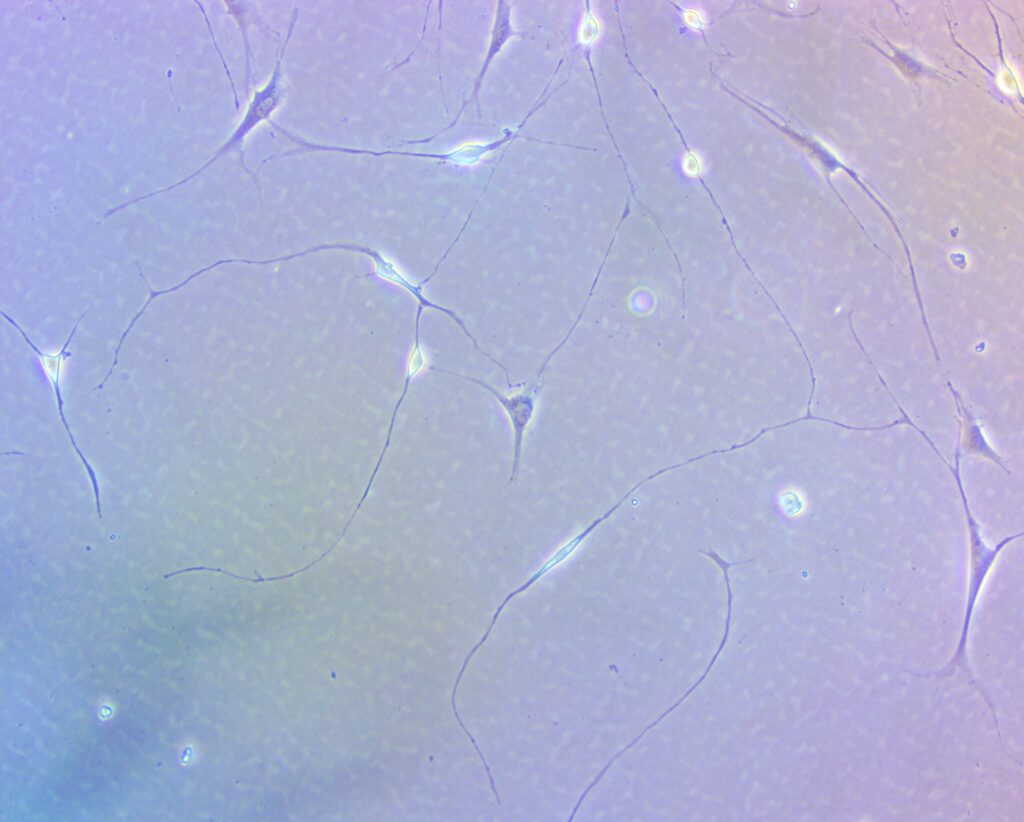
Hence our neural reprogramming method works equally well on ‘old’ fibroblasts, which are more likely to represent the patient demographics for receiving neural implants.
Long axon projections and fast growth rate is important. At a rate of 1 mm/day, it may take up to a year to a neuron implanted in the root nerve in the spinal cord to reach its muscle target located 400 mm away. So, although the implantation of such motor neurons in the spine could benefit patients with spinal cord injuries, recovery would be slow. The phrenic nerve is another interesting candidate for implantation. Originating from the C3 to C5 cervical part of the spine, this nerve is estimated between 300 and 400 mm long and innervates the diaphragm muscle required for breathing.
APPLICATION IN AMYOTROPHIC LATERAL SCLEROSIS (ALS)
In patients with ALS, many of the ~300 motor neurons constituting the phrenic nerve degenerate, leading to de-innervation of the diaphragm and respiratory failure. ALS patients that have reach that stage often require assisted respirators. In that case, grafts of autologous motor neurons in the phrenic nerve could theoretically re-innervate the diaphragm, provided, and this is important, that a drug or a cure exists to protect the implanted neurons from the devastative features of ALS. Otherwise, since the implanted neurons are autologous, they will resume ALS inevitably. To bypass a year of axon growth, it may be also possible to implant neurons closer to the diaphragm or even directly in the diaphragm, which would then require using electrodes for stimulation. But regardless of the implantation site, without a drug to protect the implant, implanted neurons will degenerate and die with certainty. This drug doesn’t exist yet; however, many laboratories are investigating promising therapeutic pathways. There are also no guaranties that such drug alone would be capable to totally block all the pathological effects of ALS. One such effect involves the dysregulation of TDP-43, a protein that is aggregated in the cytoplasm of neurons in 97% of all ALS cases. To prevent such aggregation to take place in our neurons, we are considering bioengineering an intracellular protection system against TDP-43 aggregation and integrate this system directly within the neurons produced in vitro. This protection system will be based on gold nanoparticles specifically targeting TDP-43 aggregates. We hope that “ALS-resistant” or more specifically “TDP-43 resistant neurons”, with the help of future therapeutics targeting ALS, will constitute a powerful combination to cure ALS.